Understanding Intrathecal Therapy
May 4th, 2022 Education, Understanding Intrathecal Therapy
How Intrathecal Therapy Delivers Morphine Sulfate for Continuous Pain Relief
What is Intrathecal Therapy?
Intrathecal Therapy (ITT) is the treatment and management of chronic pain through targeted drug delivery. Medication is introduced directly into the fluid around the spine, known as the intrathecal space, for faster, more powerful relief compared to oral treatments. The medication, in this case, morphine sulfate, is administered through a continuous microinfusion device (such as a pump) and doesn’t have to work its way through your body the way oral drugs do.
Intrathecal therapy can be used to treat chronic back and neck pain, sciatica, abdominal pain, pain as a result of a failed back or neck surgery, cancer pain, and reflex sympathetic dystrophy or complex regional pain syndrome.*
Getting Started with ITT
In order to be treated with injectable morphine sulfate through intrathecal therapy, the patient needs to undergo a relatively quick and simple procedure to implant the medication pump.
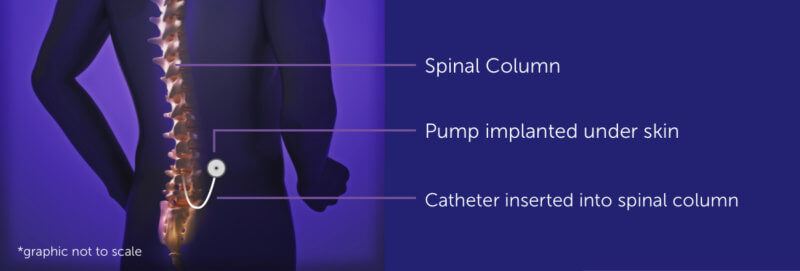
During the surgery, the microinfusion pump – a round, metal device about the size of a hockey puck* – is implanted into the abdomen, just under the skin. A catheter runs from the pump to the space around the spinal cord to deliver medication directly into the fluid around the spine in order to target specific receptors in the spinal cord. The space and fluid surrounding the spine are known as the intrathecal space, hence the name intrathecal therapy.
The morphine sulfate pump is then programmed specifically to the patient and their needs, as determined by their doctor or medical provider. Designed to slowly release medication over a period of time, the pump can either deliver the same amount of morphine sulfate each time or release different amounts at different times of the day. Dosage and timing are decided by the doctor prior to the implantation but can increase or decrease as needed.
A nurse or doctor will closely monitor the amount of morphine sulfate in the pump to ensure a patient never has an empty pump and to prevent morphine withdrawal. When it’s time to refill the device, a nurse or doctor inserts a needle through the patient’s skin and into the fill port on the top of the pump. The pump continues to provide medication without interruption to the patient.
The Benefits of Continuous Dosing with Intrathecal Therapy
Because morphine sulfate is always being released through the pump, intrathecal therapy is also known as continuous dosing. The idea of having opioids consistently running through their body might give patients pause, but treatment is an incredibly safe and more convenient way to consistently manage pain, as the relative potency (mg) of intrathecal drugs is 0.1 versus oral which is 30. That means the ratio is 300:1 from oral to intrathecal; in other words, you’d need 300 oral opioids to get the same effect as 1 dose of intrathecal morphine sulfate.
ITT vs. Other Chronic Pain Medications and Therapies
The biggest benefit of intrathecal therapy is it allows for ongoing pain relief. Patients don’t have to worry about the medicine wearing off and their pain rearing its ugly head again. Additionally, thanks to the targeted delivery of medication at the pain site, patients experience a substantial increase in pain relief compared to other therapies. With less pain and improved mobility, patients are better able to perform daily tasks and activities, resulting in more independence.
When patients use a non-compounded injectable morphine sulfate, such as FDA-approved MITIGO™, for chronic pain relief, they can rest assured their relief and symptoms won’t change from dose to dose. Compounded drugs can vary in potency and dosage, depending on how they are mixed. But, because non-compounded drugs don’t need to be mixed with anything, potency and dosage don’t often fluctuate and patients can expect the same results from each refill of their pump.
Other benefits of intrathecal therapy include:
- Less invasive than dorsal column stimulation or corrective surgery
- Cheaper than Conventional Medical Management over time and decreases healthcare utilization
- Less dose escalation over time
- Decrease in/elimination of oral drug use
Intrathecal therapy not only provides the highest amount of relief to a patient but also mitigates the risk of opioid dependency due to its targeted therapy.
The Preferred Opioid Option
When comparing intrathecal injectable morphine sulfate to oral opioids, the former is a preferred choice for pain management and is consistently more effective.
Advantages of using intrathecal injectable via a pump vs. oral morphine include:
- Better control and measurement of dosage and use
- Less chance of misuse, abuse, or overuse
- A lower amount of medication needed
- Less dosage escalation over time
- Decreased risk of experiencing adverse side effects
For a more in-depth dive into the benefits of intrathecal therapy over oral medication, check out our blog post “Morphine Sulfate Injection: The Preferred Chronic Pain Treatment Option.”
Ready to Make the Switch?
If you suffer from chronic pain and aren’t getting relief with your current treatment, it’s time to talk to your doctor about the possibility of switching to intrathecal therapy.
If you’re a medical provider with a patient who could benefit from intrathecal therapy and you’re interested in learning more, sign up for one of our education programs or contact us to book a meeting with our team.
Contact us for more information on MITIGO
Important Risk Information
INDICATIONS AND USAGE
MITIGO™ (Morphine Sulfate Injection, USP – Preservative-free) is an opioid agonist, for use in continuous microinfusion devices and indicated only for intrathecal or epidural infusion in the management of intractable chronic pain severe enough to require an opioid analgesic and for which alternative treatments are inadequate.
IMPORTANT RISK INFORMATION
WARNING: RISKS WITH NEURAXIAL ADMINISTRATION; LIFE-THREATENING RESPIRATORY DEPRESSION; RISK OF ADDICTION, ABUSE, AND MISUSE; NEONATAL OPIOID WITHDRAWAL SYNDROME; and RISKS FROM CONCOMITANT USE WITH BENZODIAZEPINES OR OTHER CNS DEPRESSANTS
See full prescribing information for complete boxed warning.
- Single-dose neuraxial administration may result in acute or delayed respiratory depression up to 24 hours. Because of the risk of severe adverse reactions when MITIGO is administered by the epidural or intrathecal route of administration, patients must be observed in a fully equipped and staffed environment for at least 24 hours after the initial dose.
- Serious, life-threatening, or fatal respiratory depression may occur. Monitor closely, especially upon initiation or following a dose increase. Patients must be observed in a fully equipped and staffed environment for at least 24 hours after each test dose and, as indicated, for the first several days after surgery.
- MITIGO exposes users to risks of addiction, abuse, and misuse, which can lead to overdose and death. Assess patient’s risk before prescribing and monitor regularly for these behaviors and conditions.
- Prolonged use of MITIGO during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated. If prolonged opioid use is required in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available.
- Concomitant use of opioids with benzodiazepines or other central nervous system (CNS) depressants, including alcohol, may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing for use in patients for whom alternative treatment options are inadequate; limit dosages and durations to the minimum required; and follow patients for signs and symptoms of respiratory depression and sedation.
CONTRAINDICATIONS
- Significant respiratory depression
- Acute or severe bronchial asthma in an unmonitored setting in absence of resuscitative equipment
- Concurrent use of monoamine oxidase inhibitors (MAOIs) or use of MAOIs within the last 14 days
- Known or suspected gastrointestinal obstruction, including paralytic ileus
- Hypersensitivity or intolerance to morphine
Neuraxial administration of MITIGO is contraindicated in patients with:
- Infection at the injection microinfusion site
- Concomitant anticoagulant therapy
- Uncontrolled bleeding diathesis
- The presence of any other concomitant therapy or medical condition which would render epidural or intrathecal administration of medication especially hazardous.
WARNINGS AND PRECAUTIONS
- Risk of Inflammatory Masses: Monitor patients receiving continuous infusion of MITIGO via indwelling intrathecal catheter for new signs or symptoms of neurologic impairment.
- Risk of Tolerance and Myoclonic Activity: Monitor patients for unusual acceleration of neuraxial morphine, which may cause myoclonic-like spasm of lower extremities. Detoxification may be required.
- Life-Threatening Respiratory Depression in Patients with Chronic Pulmonary Disease or in Elderly, Cachectic, or Debilitated Patients: Monitor closely, particularly during initiation and titration.
- Adrenal Insufficiency: If diagnosed, treat with physiologic replacement of corticosteroids, and wean patient off of the opioid.
- Severe Hypotension: Monitor during dosage initiation and titration. Avoid use of MITIGO in patients with circulatory shock.
- Risks of Use in Patients with Increased Intracranial Pressure, Brain Tumors, Head Injury, or Impaired Consciousness: Monitor for sedation and respiratory depression. Avoid use of MITIGO in patients with impaired consciousness or coma.
ADVERSE REACTIONS
Most serious adverse reactions were respiratory depression, apnea, circulatory depression, respiratory arrest, shock, and cardiac arrest. Other common frequently observed adverse reactions include: sedation, lightheadedness, dizziness, nausea, vomiting, and constipation.
USE IN SPECIFIC POPULATIONS
- Pregnancy: May cause fetal harm.
- Hepatic and Renal Impairment: May affect the metabolism and excretion of MITIGO.
To report SUSPECTED ADVERSE REACTIONS, contact Piramal Critical Care, Inc. at 1-888-822-8431 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
For additional Important Risk Information, including boxed warning, see enclosed Full Prescribing Information.
INDICATIONS AND USAGE
MITIGO™ (Morphine Sulfate Injection, USP – Preservative-free) is an opioid agonist, for use in continuous microinfusion devices and indicated only for intrathecal or epidural infusion in the management of intractable chronic pain severe enough to require an opioid analgesic and for which alternative treatments are inadequate.
IMPORTANT RISK INFORMATION
WARNING: RISKS WITH NEURAXIAL ADMINISTRATION; LIFE-THREATENING RESPIRATORY DEPRESSION; RISK OF ADDICTION, ABUSE, AND MISUSE; NEONATAL OPIOID WITHDRAWAL SYNDROME; and RISKS FROM CONCOMITANT USE WITH BENZODIAZEPINES OR OTHER CNS DEPRESSANTS
See full prescribing information for complete boxed warning.
- Single-dose neuraxial administration may result in acute or delayed respiratory depression up to 24 hours. Because of the risk of severe adverse reactions when MITIGO is administered by the epidural or intrathecal route of administration, patients must be observed in a fully equipped and staffed environment for at least 24 hours after the initial dose.
- Serious, life-threatening, or fatal respiratory depression may occur. Monitor closely, especially upon initiation or following a dose increase. Patients must be observed in a fully equipped and staffed environment for at least 24 hours after each test dose and, as indicated, for the first several days after surgery.
- MITIGO exposes users to risks of addiction, abuse, and misuse, which can lead to overdose and death. Assess patient’s risk before prescribing and monitor regularly for these behaviors and conditions.
- Prolonged use of MITIGO during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life-threatening if not recognized and treated. If prolonged opioid use is required in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available.
- Concomitant use of opioids with benzodiazepines or other central nervous system (CNS) depressants, including alcohol, may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing for use in patients for whom alternative treatment options are inadequate; limit dosages and durations to the minimum required; and follow patients for signs and symptoms of respiratory depression and sedation.
CONTRAINDICATIONS
- Significant respiratory depression
- Acute or severe bronchial asthma in an unmonitored setting in absence of resuscitative equipment
- Concurrent use of monoamine oxidase inhibitors (MAOIs) or use of MAOIs within the last 14 days
- Known or suspected gastrointestinal obstruction, including paralytic ileus
- Hypersensitivity or intolerance to morphine
Neuraxial administration of MITIGO is contraindicated in patients with:
- Infection at the injection microinfusion site
- Concomitant anticoagulant therapy
- Uncontrolled bleeding diathesis
- The presence of any other concomitant therapy or medical condition which would render epidural or intrathecal administration of medication especially hazardous.
WARNINGS AND PRECAUTIONS
- Risk of Inflammatory Masses: Monitor patients receiving continuous infusion of MITIGO via indwelling intrathecal catheter for new signs or symptoms of neurologic impairment.
- Risk of Tolerance and Myoclonic Activity: Monitor patients for unusual acceleration of neuraxial morphine, which may cause myoclonic-like spasm of lower extremities. Detoxification may be required.
- Life-Threatening Respiratory Depression in Patients with Chronic Pulmonary Disease or in Elderly, Cachectic, or Debilitated Patients: Monitor closely, particularly during initiation and titration.
- Adrenal Insufficiency: If diagnosed, treat with physiologic replacement of corticosteroids, and wean patient off of the opioid.
- Severe Hypotension: Monitor during dosage initiation and titration. Avoid use of MITIGO in patients with circulatory shock.
- Risks of Use in Patients with Increased Intracranial Pressure, Brain Tumors, Head Injury, or Impaired Consciousness: Monitor for sedation and respiratory depression. Avoid use of MITIGO in patients with impaired consciousness or coma.
ADVERSE REACTIONS
Most serious adverse reactions were respiratory depression, apnea, circulatory depression, respiratory arrest, shock, and cardiac arrest. Other common frequently observed adverse reactions include: sedation, lightheadedness, dizziness, nausea, vomiting, and constipation.
USE IN SPECIFIC POPULATIONS
- Pregnancy: May cause fetal harm.
- Hepatic and Renal Impairment: May affect the metabolism and excretion of MITIGO.
To report SUSPECTED ADVERSE REACTIONS, contact Piramal Critical Care, Inc. at 1-888-822-8431 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
For additional Important Risk Information, including boxed warning, see enclosed Full Prescribing Information.